Breast Cancer
Home / Service /Breast Cancer
Breast Surgeon in Pune – Dr. Amol Dumbre
Breast Surgeon in Pune – Dr. Amol Dumbre
Dr. Amol Dumbre is one of the leading Breast Cancer Specialist in Pune. He has been practicing in Pune as a surgical oncologist for the last ten years. He is the best Breast Cancer Specialist in Pune and works as a senior cancer specialist at Noble Hospital and Ruby Hall Clinic. Both Hospitals are very popular and trustable. He has trained and done his research fellowship from the Tata Memorial Hospital. During this period he was trained extensively in many aspects of cancer surgery. He was also involved in teaching programs. He is the best Breast Surgeon in Pune who is also a fellow in Minimal access surgery which is breast surgery. His main area of interest is breast cancer surgery.
Breast Cancer
Breast cancer is the most common of all cancers and is the leading cause of cancer deaths in women . Worldwide, accounting for >1.6% of deaths and case fatality rates are highest in low-resource countries. A recent study of breast cancer risk in India revealed that 1 in 28 women develop breast cancer during her lifetime. This is higher in urban areas being 1 in 22 in a lifetime compared to rural areas where this risk is relatively much lower being 1 in 60 women developing breast cancer in their lifetime. In India, the average age of the high-risk group in India is 43-46 years. In the west where women aged 53-57 years are more prone to breast cancer.
What Are Symptoms And Signs Of Breast Cancer?
- A lump felt by the patient or during routine physical examination or mammography.
- Less commonly, the presenting symptom is thickening in the breast. Paget’s disease of the nipple presents with skin changes, including erythema, crusting, scaling, and discharges.
- A few patients with breast cancer present with signs of metastatic disease (eg, pathologic fracture, pulmonary dysfunction).
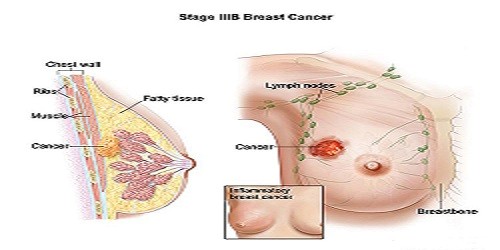
During a physical examination, a lump is felt distinctly different from the surrounding breast tissue. More advanced breast cancers are characterized by fixation of the lump to the chest wall or to overlying skin, by satellite nodules or ulcers in the skin. Matted or fixed axillary lymph nodes suggest tumor spread. Inflammatory breast cancer is characterized by diffuse inflammation and enlargement of the breast, often without a lump, and has a particularly aggressive course.
Risk Factors
The risk factors influencing breast cancer risk are broadly classified into two factors:
- Modifiable factors: The modifiable risk factors are BMI, age at first childbirth, number of children, duration of breastfeeding, alcohol, diet, and number of unsuccessful pregnancies ( abortions).
- Non – Modifiable factors: The non-modifiable risk factors are age, gender, number of first degree relatives suffering from breast cancer, menstrual history, age at menarche and age at menopause.
Screening
Pathology
Pathophysiology
Diagnosis
Radiology
Magnetic Resonance Imaging
Pathology
Treatment
Breast cancer can be treated using
- a multimodality approach of surgery
- chemotherapy
- radiotherapy
- targeted therapy
- hormonal therapy
The treatment options vary as per the stage of the tumor. Dr. Amol Dumbre is one of the leading Breast Cancer Specialist in Pune. He has been practicing in Pune as a Breast Cancer Specialist for the last ten years. He is the best Breast Cancer Specialist in Pune
Surgical options
- BreastConservation Surgery.
- Modified Radical Mastectomy.
- Mastectomy with Reconstruction.